
A few days ago, I donated a kidney to my dad. Because it might be helpful to other donors, I’m writing down what my experience was like here- all the way from learning about my dad’s disease to walking out of the hospital with one kidney. I’ve included notes on the prep work, what the pain has been like, and what sort of medications I’ve been taking.
Needing a Kidney
Ten years ago, my parents told me that my dad’s kidney health was declining and becoming an issue. I told my dad, “Hey, you need a kidney, I got an extra.” He assured me that he didn’t need one and that he was going to take some medication and make some lifestyle changes.
That worked for about seven years, but then three years ago I talked with my folks again and they said that his kidney health had declined so badly that he was going to need a transplant, dialysis, or both.
The Numbers
One of the primary scores that determine the need for donation is what’s known as GFR or Glomerular Filtration Rate. It’s a measure of how much blood your kidneys can filter per minute.
- At 20 GFR kidney function you can get on a donor list to be in line to get a cadaver kidney from someone who has died. You may want to get on multiple state lists.
- At 17 GFR kidney function Medicare will pay for the transplant.
- At 15 GFR kidney function you need to start dialysis.
My dad had dropped beneath that 20 threshold, but wasn’t to 15 yet.
My Dad Didn’t Want My Kidney
My dad didn’t want my kidney. Though he needed it, he didn’t want to do anything that might impact my health. He told me in one conversation that everyone’s life is finite and that it might just be his time to die. That’s a hard thing to hear from someone you love.
Our family had lots of conversations about me donating and dad receiving my kidney and we were able to sway him to being open to donation from me.
Racing Against Dialysis
I had talked with several people in the medical community and they explained to me that dialysis was a rubicon of sorts. Once my father began doing dialysis, his mortality rate would go up and he would be more likely to have cardiovascular issues, a stroke, or cancer.
Additionally, any transplant operation after dialysis would be riskier and more difficult for him to recover from.
Because of these factors, it was really important that we get him a kidney before he started dialysis.
Initial Labs
We worked with the University of Utah Hospital, the closest transplant center to my parent’s farm.
I live in Portland, Oregon and once we contacted the transplant center they assigned me to a donor coordinator named Shalei.
Shalei and I spoke over the phone and she told me that as a donor all of my medical costs were covered, but that travel expenses or wage loss due to recovery was not paid for. She said there were scholarships available for these and she could help me apply if that was something I needed help with.
She explained to be approved for transplant I would need to:
- Complete blood and urine labs.
- Attend a donor education class.
- Speak with a social worker assigned to me.
I received a lab order and I took it to the hospital closest to me. In most cases, I believe donors take the order to businesses that specialize in this kind of outpatient lab work, but a hospital was easiest for me. (Note that not all hospitals will do the labs. My insurer is an HMO named Kaiser and they refused to do the labs for an entity not part of the Kaiser organization.)
The labs themselves were pretty simple:
- I had to do a 24 hour urine collection prior to giving blood. Starting when I woke up, I peed into a large container and had to keep it in our refrigerator for 24 hours.
- The next morning I took my big jug of pee to the lab and they took it and drew a bunch of vials of blood.
- They also had me do a urine sample at the lab.
Afterward, I called up Shalei and gave her the number of the hospital. She took care of all the billing and making sure the labs were transmitted to the University of Utah.
Shalei had me sign up for an online service called MyChart. MyChart enabled me to get messages from the transplant team and see my labs when they were completed. It’s a service that is separate from any one hospital and my HMO was able to access MyChart and see the results from the labs as well.
The donor education class was a 30 minute class delivered over a teleconference phone call. Shalei provided me a list of scheduled classes and I selected one that worked for my schedule. Then, she sent me a PDF to review during the class. On the scheduled day, I called a number and walked through the PDF with the donor education teacher. At the end, the teacher asked some questions to make sure everyone on the call understood what was involved in donation and what the ramifications were.
The life expectancy for donors is better than the national average. Meaning donors tend to live longer than non-donors. However, this is because donors are healthier than normal people. If you could hypothetically compare your donating versus non-donating version of yourself the non-donating would be healthier.
Post donation, your remaining kidney grows in size to a “super kidney” and makes up much of the loss function so that you still have better than 100% kidney function.
I also had a call with my social worker. The social worker wanted to know:
- That I was psychologically healthy.
- That I wasn’t being coerced or bribed into donating.
- That I had a support network at home and the means to take time off from work after donation.
Paired Exchange
Once I completed the above tasks, the transplant team confirmed that I was a match for my dad as a donor.
However, this isn’t always the case. Sometimes a donor comes from outside the family or the blood doesn’t match up. In those events, the transplant team sets up what is called a paired exchange.
For a paired exchange, they use a registry of people in similar circumstances and find a donor and recipient who match up with your blood and your recipients blood and schedule a set of surgeries so that the pair of matches exchange kidneys (a stranger gets your kidney and your recipient gets a donor kidney from a stranger).
Final Tests
After getting through the above tasks, the transplant team wanted to see me in person for a final round of labs and questions.

I flew out to Salt Lake and went to the transplant clinic at the University of Utah.
They drew my blood again, had me do another urine sample, and had me talk to several people on the team:
- The transplant surgeon
- My social worker.
- My donor coordinator Shalei.
- A nephrologist (kidney specialist).
- A dietician.
All these people explained what would happen in surgery and how my life would change post surgery.
Additionally, they had me do abdominal x-rays and a CT scan.
I never had a CT scan before. It’s a machine with a bed that has a large open ring at the end. They hook you up to an IV and then pump a radiated isotope solution through your veins. You feel warm and a little like you just wet your pants. Almost immediately after the isotope starts flowing you get a chalky flavor in your mouth. Once they have the solution in your veins they hit a button from the control room and the bed slides back and forth through the ring. The whole process takes about twenty minutes and is only mildly uncomfortable. You pee out the isotope within 24 hours (not that you can see it.)
They also explained to me again that if I wanted to donate, I had the right to change my mind at any point in the process. I could literally be on the bed getting wheeled in to the operating room and say, “Nope, I changed my mind,” and they would stop the surgery and tell everyone that something had come up that prevented me from being able to donate. In other words, no one would know that I changed my mind.
Finally, they showed me their transplant success rates as compared to the national averages.
The clinic took a little over half a day and at the end of it, they told me that the surgery team met once a week and would either clear me for surgery or bar me from donating.
What I Had to Do That You Probably Won’t
My dad has a rare form of the disease Alports. In typical Alports, women are disease carriers and men are afflicted with the symptoms. Most men die before they reach the age of thirty.
In my dad’s version, this isn’t the case. Instead, my aunt was afflicted with the symptoms and had to get a transplant when she was 40. My dad made it all the way until he was 67. My other aunts and uncles weren’t seriously affected by the symptoms.
Because the disease was something the transplant team hadn’t seen before, they were very careful accepting me as a donor.
In addition to the normal donor process, I had to go see two eye specialists that imaged my eyes and ran various tests on me (Alports shows up in your eyeballs for some reason). I also had to fly back to Salt Lake City a second time and get a kidney biopsy. I’ll spare you the details, but suffice to say that the kidney biopsy was painful.
After these tests, they cleared me for donation.
But Then My Dad Got Better
After getting cleared, I wanted to do the surgery and have it in the rear view mirror- but my dad didn’t. He wanted to postpone the surgery until the fall and summer harvest was over (he’s a farmer.)
In the meantime, my dad made lots of positive lifestyle changes. He began working out at the YMCA on a regular basis doing their circuit training. He also changed his diet to a more strict version.
At the end of the summer, his kidney function scores had actually improved.
We continued to postpone surgery and his scores climbed a bit further and then plateaued.
But Then My Dad Got Worse
Two years went by and I began to think that he might get a cadaver kidney because most people get a kidney between two and three years after they’re accepted to the donor list.
But then my mom reached out six months after the two year mark and told me that my dad’s scores were starting to drop again.
I emailed Shalei, “I think we’re going to need to schedule the surgery soon.” She told me that they had changed the rules so that living donors had to redo their labs every year and I had passed beyond that mark and had to get them again.
Drinking and Smoking
When I had first done the labs I was a teetotaller and hadn’t had a drop of alcohol in years. In the time since, I started to drink socially again.
For the person donating, they don’t want you drinking more than 1 – 2 drinks a week. That means beers, glasses of wine, or shots of liquor- not a couple Long Island Teas a week. Shalei told me that I needed to be careful to stay within this range or it might impact my being able to donate.
Additionally, you can’t do your labs within 30 days of smoking and they don’t want you smoking or taking tobacco products at all leading up to surgery.
I don’t smoke except for one to two cigars a year. However, I had just hung out with some friends who wanted to smoke hookah after a concert. Because of that, I wasn’t able to do my labs until 30 days had passed.
Rescheduling Surgery
My redoing of the labs were very similar to the first time- first doing them remote and then flying to Salt Lake again. However, the second time through Salt Lake I got a call from Shalei at the airport on my way home. She told me that they had found a granuloma in my lungs in my CT scan. They didn’t think it was cancer, but it might impact my donation.
Later that week the transplant team met to determine whether I could donate and they decided that, though I was cleared for surgery, they wanted to see a CT scan of my chest first (for normal donation it’s just your abdomen.) Shalei penciled in a tentative surgery for December 19th.
Meanwhile, I scheduled a CT scan at the local hospital and they found three granulomas in my chest.
A week went by and Shalei called to tell me that the team had met again and they weren’t going to let me donate on the 19th unless a pulmonologist reviewed the CT scan and cleared me.
I tried a couple different avenues to get the pulmonologist review, but couldn’t get it done in time for the surgery so we delayed surgery. In the meantime though, the University had a radiologist and a pulmonologist review the scans and they determined the granulomas were not going to be an issue and cleared me a week before I would have had the surgery.
As you can probably tell at this point, they’re extremely careful about only accepting healthy donors that won’t be impacted by losing a kidney.
They told me that on the off chance that something developed and I needed a kidney that, as a donor, I would be bumped to the front of the list for deceased transplants.
Deceased Donors and Dialysis at the 11th Hour
Over Christmas, my dad got a call from the hospital that he had come up on the deceased donor list and to be on standby to fly to Salt Lake- they might have a kidney for him. This proved to be a false alarm.
A few days later, at the beginning of 2020, we rescheduled surgery for February 4th. Shortly after this, my dad did his quarterly blood work and found out that he had dropped several points and needed to go on dialysis. But because surgery was only a month away, his nephrologist thought he could hold off and still be okay.
Then a few weeks later, he got another call- they thought they had another kidney for him. He had been on the deceased donor list for almost three years exactly. He and my mom hopped in a car and drove four hours to Salt Lake. The transplant team told him to head right into the hospital and up to the operating room. However, when they arrived, the receptionist stopped him at admission and told him to wait. After a couple of hours, someone on the transplant team came to tell him that he wasn’t going to get a deceased kidney after all. Apparently, they thought a donor in the hospital was going to die but didn’t.
He was ready for this eventuality because they tell recipients on the deceased donor list that until you wake up from surgery with a kidney in you, you don’t have that kidney.
How I Felt About All This
For me, all of this was a bit weird.
On one hand, I didn’t want to donate if I didn’t have to. I workout religiously and I wasn’t looking forward to the long and slow recovery period. Other donors had reported it taking up to a year before they felt normal again and I anticipated it would probably take me at least two years to get back to my physical condition. Bummer. Plus, who wants to do surgery?
But on the other hand, if I donated my dad would get what they call a “warm kidney.” We would literally be in operating rooms next to each other and one surgery team would walk it over to the other after pulling it out of me. Most donations are from people dying and the kidneys have to be on ice and flown to the transplant center. Warm kidneys function better and improve the recipient’s health over the long term. Additionally, if I gave my dad a kidney, he’d be off the deceased donor list and the next person would get bumped up in line and receive a kidney that much sooner. I would accelerate the donor list by one person and likely save a stranger’s life at some point.
Final Check
A week before surgery, both my dad and I went into get our blood drawn and provide urine samples on the same day, within hours of each other, and hundreds of miles apart. It’s a final check to make sure that your blood still matches.
Transplant Surgery Arrives
Surgery was scheduled for Tuesday. The Friday before I received several phone calls from the transplant team. They told me that I would be in the hospital for 2 – 3 days post surgery and that I would be discharged with tylenol, tramadol, and a stool softener (anesthesia blocks you up and they don’t want you straining post surgery.) They told me to drink plenty of water the day before, but to have a light meal in the evening and to not have anything after midnight the night before: no water, no lozenges, no gum. All of that stimulates the stomach and they can’t safely do surgery with your GI system in gear.
The day before surgery, they called me up with my surgery time. I had to be at the hospital at 5:45 AM and surgery would start around 7:30. It would take 2 – 4 hours for me and 3 – 5 hours for my dad.
I flew into Salt Lake with my wife that night and my folks picked us up at the airport and took us to the hotel.
We got a few hours of sleep and then all piled into a car and headed over to the hospital.
We checked into admissions at the lobby and they sent us up to the operating room waiting area where we checked in again.

The waiting area was full of families getting ready for their loved ones to head into surgery. They gave my wife and mom a color coded card and showed how it reflected a monitor on the wall next to the operating area doors. The monitor had our last names and they would change color as we were moved into surgery prep, surgery, surgery completion, surgery recovery, and then into our post operation rooms.
After waiting about fifteen minutes, they called my dad back. A few minutes later, they called my name and my wife and I followed a nurse back to a pre-operation room. I changed out of my street clothes and into a gown and laid in a bed while they took my vitals. They put this weird blanket on me that was a thin plastic sheet. They hooked it up to an air hose and it inflated like a pool toy that was filled with hot air.
A member of the surgery team came by and told me that I’d be heading into the operating room about thirty minutes before my dad.
Then an anesthesiologist came by and inserted an IV. I’m vasovagal, which means that I have a psychosomatic reaction to certain things. I’ll black out sometimes when I’m getting blood drawn and can get nauseated and vomit. Though it didn’t hurt, I started to have a reaction when the anesthesiologist inserted the IV into the back of my hand. They laid me down flat and the feeling passed.
After that, I read a book until 7:30 when they came for me. My wife took my clothes and belongings and they wheeled me out into the hallway
It was a bit odd, because I was so into my book and a little sleep deprived. Suddenly, I wasn’t in the story and I was on my way to surgery!
I wasn’t nervous, just feeling tired and weird, but the anesthesiologist said over my shoulder, “I’m going to give you a little something to relax.”
Almost immediately, I felt like I had two glasses of wine. Not buzzed, but very relaxed. “That’s nice,” I told her, “I like that.”
They wheeled me into the operating room. It was a large open room with a table in the center and shelving and counters on the wall. It was a bit dark in the room, but next to the table I could see several large lights above me, waiting to be turned on.
A few seconds after they stopped my bed, the anesthesiologist told me, “Okay, I’m going to cover your face with this mask. It’s going to feed you oxygen.” She put the mask around my head and as she did this she said, “Now I’m going to put you to sleep.”
And as she said that I went to sleep.
Sleep and Waking
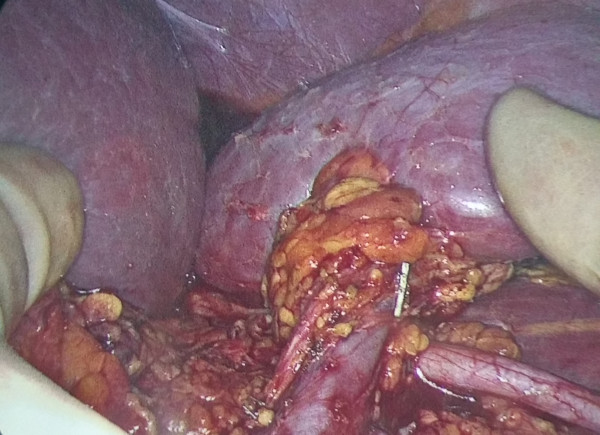
My Dad’s New Kidney
I slept really deeply while they operated on me. I didn’t have any dreams, but have a vague recollection of voices above me.
I woke up in a large room with beds lining the walls and someone talking to me. Being the polite guy that I am, though I wanted to keep sleeping, I opened my eyes. This guy was telling me about all the twists and turns of his life, how he was older than other nurses and late getting into nursing.
“Do you regret all those twists and turns,” I asked him.
“No,” he laughed, “I wouldn’t have it any other way. You can call me Rick the Nurse. How’s your pain?”
“Four or five,” I told him, responding in the healthcare 1 – 10 pain scale. It was uncomfortable, but not overpowering.
“Okay, let’s bring that down,” he said and shot some stuff into my IV.
“How about now?” he asked a few minutes later.
“Three? Two?” I responded.
“Good,” he said, “You’re in the PACU. We’ve got acronyms for everything, but basically it’s the post surgery care area. You did great. We’ll keep you here until we get you a room. There’s a chance that you’ll have to board here because some days we go ‘code red’ and everything fills up and today is looking like one of those days. We’ll try and get you a room.”
I went back to sleep.
“Good news my man,” Rick the Nurse woke me back up, “Your dad is coming out and we’ve got a space open right next to you. How lucky is that?”
I saw my dad get wheeled into the bed area on my left. I couldn’t see his face, but recognized his hand when I turned my head.
I slept and woke up and saw a doctor talking to my dad.
The doctor straightened and turned around to me.
“I’m your father’s surgeon,” the doctor told me. “Your dad really needed that kidney and you gave him a great one. He should have been on dialysis.”
“How’s he doing?”
“He did well in the surgery, but his heart has a little bit of arrhythmia. This happens sometimes because of all the fluid we pump into them during the operation. We’re going to move him to ICU as a precaution.”
Not good. They were saying his heart rate was inconsistent and a bit too fast- the concern being that he might have a heart attack.
My dad later told me that if the surgeons had their way they would have operated on him when his GFR score was 20. His last score, a month before donation was 14. He started at 16 three years ago, rose to 19, then dropped to 17. Over the course of six months he dropped from 17 to 16 to 14. Apparently, this is typical, where patients tend to decline in their scores very quickly as their kidneys fail.
I stared at the wall and tried to get a look at him a couple of times, but couldn’t see past the metal arm on the bed.
“Hey my man,” Rick the Nurse said, “Your wife and mom are on the way back to see you.”
A few minutes later I opened my eyes and my wife and mom were standing at the foot of the bed.
“How are you?” my wife asked.
“I’m doing good,” I said, “The pain isn’t bad. Rick the Nurse gave me some meds.”
We talked a little about the surgery and the room situation. Rick came by to let us know we had a room and it was just getting disinfected. He said that he’d let me say, “Hi,” to my dad before they moved me up to the room.
I looked over and saw my mom’s back as she stood over my dad’s bed. She turned and came over to me.
“I’m good,” I told her, “How’s dad?”
“They’re going to keep him here,” my mom said, “No ICU, which is good because they didn’t have room there. His arrhythmia is improving.”
“How are you doing?” I asked.
Tears glistened in her eyes and she said, “Thank-you so much for doing this Bud. Your father needed this kidney badly and we appreciate you going through all this.”
We chatted a little bit and then they left and told me they’d see me when I had a room.
Rick the Nurse came back with a couple of orderlies after I had dozed for awhile.
“Alright, you’re getting out of here, my man. We just need to get this catheter out of you.”
Along with the surgery itself, I wasn’t looking forward to that experience. Getting the catheter out was as painful as I anticipated, burning and intense enough for me to close my eyes, but it only lasted for a couple of seconds.
Before I left, Rick instructed the nurses to pull my bed around so that I could see my dad.
“My boy,” my dad groaned and held out his hand.
I reached across and grabbed his fingers.
“I’m doing good Pops,” I told him, “I’ll see you upstairs.”
The Hospital Stay
My wife was waiting in the room when I got wheeled in. Over the next couple of hours, a parade of different people came to check in on me and gather information.

In between visits, I would doze and wake to stare at this big white whiteboard at the foot of my bed. It had my medications on it and the next time they could be administered, who my nurse was, the assistant nurse, and the charge nurse who was responsible for the floor for that twelve hour shift.
It also listed my diet as “CLEARS,” which meant that I could only eat liquids. For dinner that night I had jello, beef broth, Hawaiian ice, and juice.
I was plugged into an IV on one hand and an oxygen monitor was taped to a finger on my opposite hand. They also gave me an ice pack to hold over my stomach.
The nurses told me to let them know when I felt well enough to walk. They said not to push it, but that they wanted me to try and stand and walk when I thought I could.
After my mom and wife had left for the evening, I decided to try and walk down to my dad’s room.
In your hospital bed, you have a remote that enables you to turn on and off the lights, the TV, and call a nurse. I hit it and my nurse, Dave, came to help me get out of bed.
He unplugged me my IV stand from the wall and I rolled onto my side and then pushed sideways with an arm to sit up and then stand.
I tottered slowly out into the hall and slowly walked the fifty feet down to my dad’s room. He had cords hanging off his neck, his arm, and from under his gown and had a small satellite next to his bed covered in electronics. He looked tired, but alert.
I asked him how he was doing, how he felt, whether he had dinner.
Standing there though, I realized I was getting a bit light headed and my dad confirmed this by saying, “You should go lay down. I’ll walk down to your room tomorrow.”
By the time I got back into my bed, I felt like I might vomit or pass out.
“Do you want me to get you anything? Anti-nausea?” asked Dave.
“No,” I mumbled, “just give me a minute.”
The feeling passed as I laid there and I told him, “I’m okay.”
“Have you peed yet?” he asked.
“No.”
“Okay, well, they want you peeing by 9:00 PM. Do you think you might be able to go?”
“Yeah,” I told him, “Maybe thirty minutes.”
Thirty minutes later I paged him and he helped me get out of bed and walk over to the bathroom.
Inside, they had a jug for me to pee into. They tracked my urine volume the entire time I was in the hospital.
I slept well through the night, except for the wake up call every four hours when the nurse or HCA would come in and take my vitals.
Around 6:00 AM the transplant team knocked on the door and flipped on the lights. They asked me how I was feeling and I told them I felt good enough to leave. They said they would plan on discharging me that afternoon and told the staff to switch me to solid food.
I still received a liquid breakfast, but the nursing staff was nice enough to have them bring me a menu and I was able to order coffee, a breakfast sandwich, and fruit.
A physical therapist came and visited me and we took a lap around the floor and stopped into say, “Hi,” again to my dad.
Both he and my wife told me that, while I may have felt like I was doing good in the PACU, I didn’t look it. He said I was white as a sheet and my wife said I was green in the face when she saw me.
Back in my room, my mom came by and told me my dad wanted me to stay another night and not rush out of the hospital. I assented and told the nurses I would stay one more night.
My donor coordinator, Shalei, came by and talked with me about discharging. She had a swag bag full of stuff from the hospital and a certificate of thanks from the transplant team (for being a living donor.) She said there was a monument in Utah for living donors and if I filled out a form, they would inscribe my name on it.
She also warned me that the first 24 hours post surgery were the toughest because the anesthesia and narcotics they pump into you in surgery wear off.

The rest of the day, I mostly hung out in my dad’s room, sitting up with a brace around my midsection that the physical therapist gave me.
In the early afternoon, I started to feel a little odd and retreated to my room. As I laid down on my bed I felt a wave of nausea pass over me. I told my wife I needed a cold cloth and she put a wet paper towel over my forehead and called for a nurse. The nurse pumped an anti-nausea into my IV and the feeling faded.
I spent the rest of the day watching the snow fall outside and responding to all the text messages and emails I was getting from friends and family wishing me and my dad well.
That evening, the staff brought in a change of hospital gowns, towels, and soap. They wrapped up my IV in a plastic bag so that I couldn’t get it wet and I hobbled over and took a shower (unassisted.)
Looking at myself in the mirror was the first time I was able to see the full damage inflicted by the surgery.

While I didn’t exactly have a six pack before, you could see my abdominal muscles. Post surgery, I looked like I had a beer gut. Shalei told me not to be alarmed by the weight gain and that they pump a bunch of fluid into you in surgery and it takes days to drain out.
I had a big vertical incision running through my belly button and two diagonal ones on my left side where they put in ports for the robot arms. They had taken my left kidney because the vein that attached to it was longer and gave them more “rope” when they reattached it to my dad.
Showering felt good and I was able to clean off and put on the new gown without needing to call for a nurse.
The second night passed similar to the first and in the morning I told the transplant team, “Okay, I’m out today for sure.”
That morning a pharmacy tech came by with my prescriptions for leaving and they had me sign some paperwork to say that I was leaving the hospital.
I shuffled out around lunch time and my mom drove my wife and I back to our hotel room.
Medications and Pain
Early in my stay at the hospital, one of the nurses told me they’d much rather be in pain than deal with nausea. The worst pain I felt in the entire experience was probably the nausea the first day after surgery and that quickly passed when they gave me drugs.
Other than that, the pain in the PACU was initially painful but tolerable but then quickly dropped to hardly noticeable after they gave me some painkillers. I did have moments of spikes of pain leaving the PACU, but the drugs they gave me quickly overcame those spikes.
The second night in the hospital, I got a little behind on my drugs and waking up to go to the bathroom was painful. It hurt enough that it was hard to breath as I moved into and out of the bed. After laying down for a few minutes though, this pain subsided.
Post surgery, all I took was tramadol, tylenol, and the anti-nausea on day one. The nurses explained that they wouldn’t give me anything stronger because of the opioid epidemic, but that I should be fine as long as I was preventative in my use of tramadol and tylenol and stayed in front of the pain.
This proved to be the case. I have only had mild discomfort the entire time post surgery and have been careful to keep on the staggered painkiller schedule with tramadol and tylenol spaced throughout the day and night.
If I were to make a recommendation to someone going into surgery, it would be to monitor their drugs along with the nurses. I think I may have missed a dose or two of tramadol that first day because I was out of my room hanging out with my family.
To put the pain into perspective, my donor coordinator said that donors had compared it to giving birth. Initially, I thought this was both bad and good. Bad, because that seems painful. Good, because people go through it all the time- no big deal.
Afterwards, I think people say that because the pain is similar to a Caesarean section. In this regard, I think it must be less than a C Section because all they pull out of you is a kidney, which is fairly small- the size of a fist. Whereas my sister-in-law had two infants squeezed out of her stomach.
I don’t think that this experience will rank in my “most painful” experiences in life. It’s not as bad as the flu, food poisonings, or some maladies with sunburn and parasites that I’ve had (travel.) What will probably stand out will be the long recovery period.
Recovery
I expected the recovery to be slower and harder than it has been. Shalei told me to expect to spend a couple weeks in bed. The only time I’ve been in bed has been to sleep. Other than that, I’ve been sitting up with a brace around my stomach.
The transplant team was okay to have me leave 24 hours post surgery, but most patients require 2 – 3 nights in the hospital. I ended up staying two and think that was a good decision, even though I probably could have left after the first night and been okay.
I have to go back to the hospital a week after surgery for a follow up where they’ll check my sutures and see how I’m doing. The sutures will dissolve on their own and I should be clear to take a hot bath in a couple of weeks without risking infection.

Exercising in slippers.
This is what my mobility looked like post surgery:
- Day 1: Sloooow walking. Not very far.
- Day 2: Sloooow walking, but able to walk all the way out of the hospital.
- Day 3: Difficulty sitting up and laying down, but better than in the hospital. Still walking like an old man, tottering back and forth.
- Day 4: Slow walking, easier getting up and down. My wife said I was sitting more comfortably and seemed closer to normal.
- Day 5: Slow walking. I was able to tie my shoes without help. I walked a quarter mile on the treadmill. Needed an extra nap in the day.
- Day 6: Slower walking. I was down to a quarter dose of the prescribed pain med. I walked a third of a mile and took an extra nap in the day. My stomach started to return to its normal size, but the bruising was still pretty bad to look at.
- Day 7: I was almost to a normal walking speed. I walked a half mile without fatigue. My stomach started to itch.
- Day 14: (Updated) I was walking at a normal speed for an hour. I felt a bit tired afterwards. The two diagonal laparoscopic incisions are starting to scar and the vertical incision was on its way too. Stomach was back to normal size.
Days 4 – 7 I’ve spent several hours writing this blog post out and going back to work at the computer.
I don’t feel like I’ve been pushing my body with exercise or pain meds, though I’ve probably been working more than I ideally would at this stage.
A caveat:
Everyone is different. I heard several stories about donors being slower than recipients in getting back on their feet and experiencing more fatigue. I’m very healthy and just approaching middle age at 38 years old. I work out six days a week, with both strength and cardiovascular training. Two to three workouts a week are very challenging. I don’t consider myself an athlete, but I’m in really good shape and stronger than the average bear. My BMI going into surgery was around 15%, pulse in the low 60’s, and normal blood pressure. My diet is mostly whole foods, with lots of vegetables, lean meats, beans, and fruit. I cook several meals a week and eat salads and soups. With that said, I frequently eat danishes, donuts, and cinnamon rolls and will eat out 2 – 3 times a week (like I said: I’m no athlete.)
In terms of long term recovery, they told me not to start exercising again for six to eight weeks. When I start, I’m supposed to ease into it. The biggest risk is over doing it and giving myself a hernia from the weakened abdominal muscles that are still healing.
Final Thoughts
Thank You Basket I Made for the Transplant Team
It took several days of writing to put this together. It’s not exactly what your experience is going to be, but I hope it’s helpful in painting a picture about what’s involved and how hard it is. I’m extremely grateful to my transplant team in helping me extend my father’s life and had a fantastic experience with the University of Utah hospital.
5 Months Later
I went into surgery thinking that it would take around a year for my body to fully recover.
This hasn’t been the case for me.
Within a month and a half I felt the same as pre-surgery and had to constantly remind myself not to lift objects heavier than a gallon of milk (the risk is a hernia from still weak abdominal walls.)
Within 2 months, I was exercising again with light weights.
By 4 months, my strength was about the same as pre-surgery.

On Top of Thielsen
My birthday was 5 months post surgery and I climbed Mt. Thielsen in southern Oregon. It’s a 9.2 mile round trip with 3200 feet elevation gain. It took me about 5 hours with a 30 minute break on the top. I’d worked out every day for the previous 2 weeks and had 6 hours of sleep.
I’m lifting heavier weights than I was pre-surgery and haven’t noticed any changes in endurance or energy levels. I feel good.
All this to say, for me, the recovery period has been pretty quick and it hasn’t impacted my quality of life.